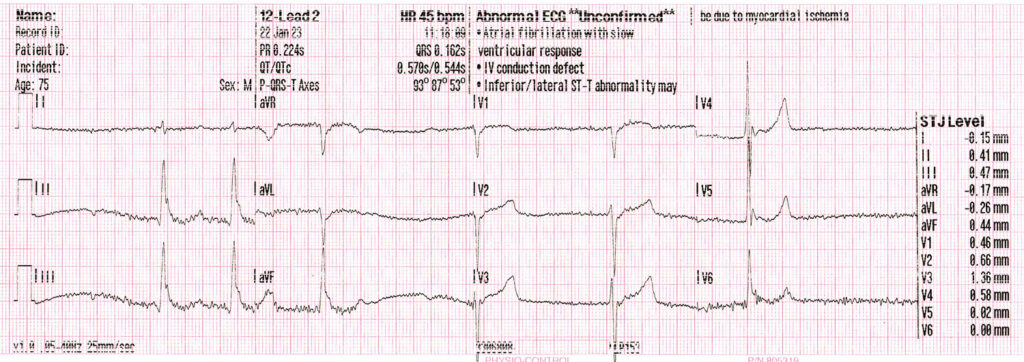
ECG #2: Hypothermia
Called to a 75 year old male, found on the floor of his home following a long lay of approx 12 hours.
Critically ill, he had a number of issues that needed correcting, hypothermic at 29°C, a blood sugar of around 2.0mmol/L, hypotensive at 66/33 with of course a reduced GCS.
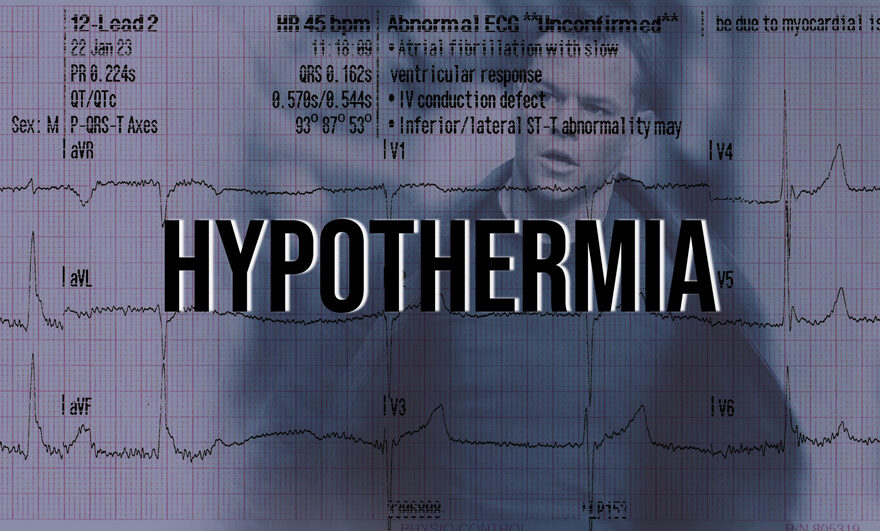
THe ECG recorded would be a great example of the effects of hypothermia:
Bradyarrhythmia: AF with slow ventricular response.
As a prehospital clinician, you mostly encounter AF + Rapid Ventricular Response (AF+RVR), aka Fast AF but rarer AF with slow ventricular response, which seems to be the case here. Bradycardia, no consistent definitive p waves, irregularly irregular.
1st Degree Heart Block
1st degree heart block is also another features of a hypothermic ECG. Perhaps p-waves can be made out in II, III, avF and avR. However these do not seem definitive and a rhythm strip does not exist to definitively diagnose such a condition.
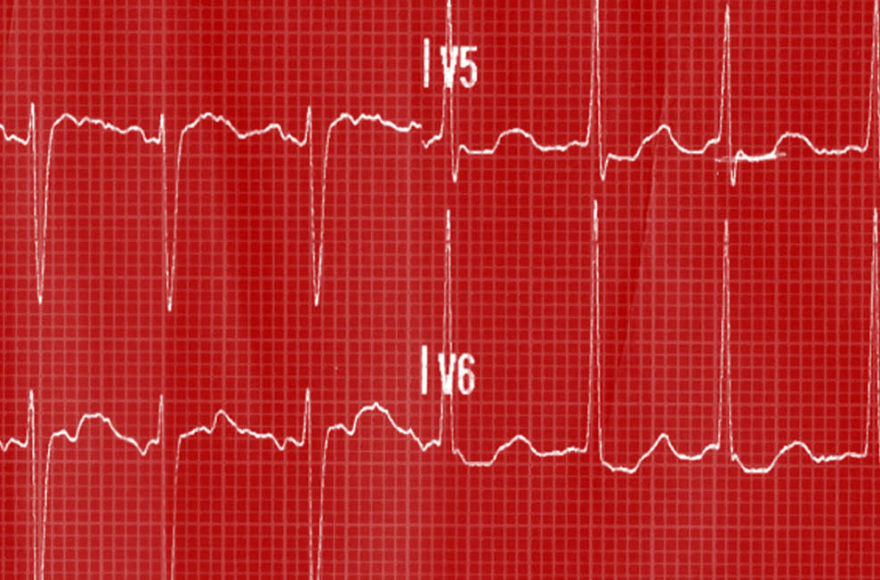
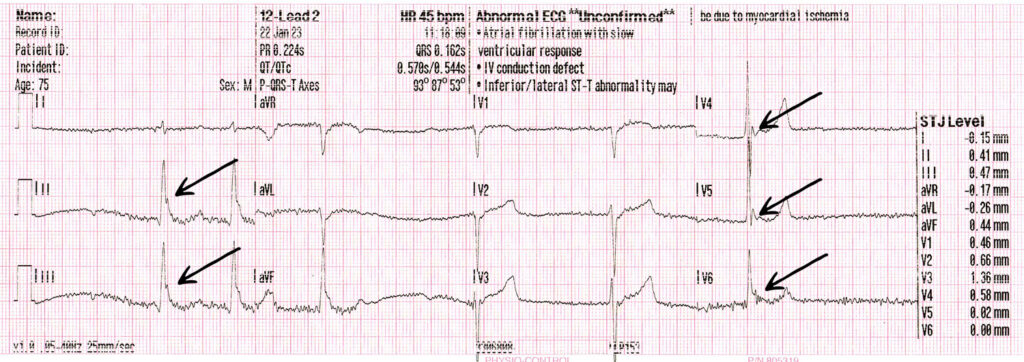
Osborn Waves
aka J-waves. And born as in birth not as in Jason Bourne. Like a lot of medical research, Osborn wasn’t the first to recognise it but was the first to claim it in his research into hypothermic dogs. He called it the ‘current of injury’. Doesn’t exist solely in hypothermic patients. Thought to be show differences between epi~ and endo~ cardial voltage gradient.
And so the patient was heated and treated and taken to hospital, leaving us with a great example of a hypothermic ECG.
References and Links
Maruyama, M. et al. (2004) “Osborn waves: history and significance.” Indian Pacing Electrophysiol Journal, Jan 1;4(1):33-9.
Yan, G. and Antzelevitch, C. (1996) “Celluar basis for the electrocardiographic Jwave.” Circulation, Jan 15;93(2): 372-9