ECG #1: Flutter
One of the concepts of prehosital ECGs I try to get across to new clinicians is that often the ECG confirms the diagnosis – that is with pt presentation, basic obs and the history, you can pretty much be confident of what the ECG might look like when it pops out of the lifepak.
The case
And so I was called to an 86 year old who have been complaining of palpitations, shortness of breath and a little bit of chest pain.
I felt her pulse and it was regular and running at around 130 bpm.
In my head I briefly thought of various ECG differentials: SVT, Fast AF, Flutter. Maybe there are more (PE, STEMI etc) but these were the main ones that popped into my head.
SVT is faster, AF is irregular so I was looking at either sinus tachy or flutter. She didn’t look particularly unwell and not many septic patients c/o chest pain and palpitations as their initial symptoms. So therefore it’s reasonable to expect flutter is the cause. Added to which it’s 130 bpm is not far from the more common flutter rate of 150bpm.
The ECG
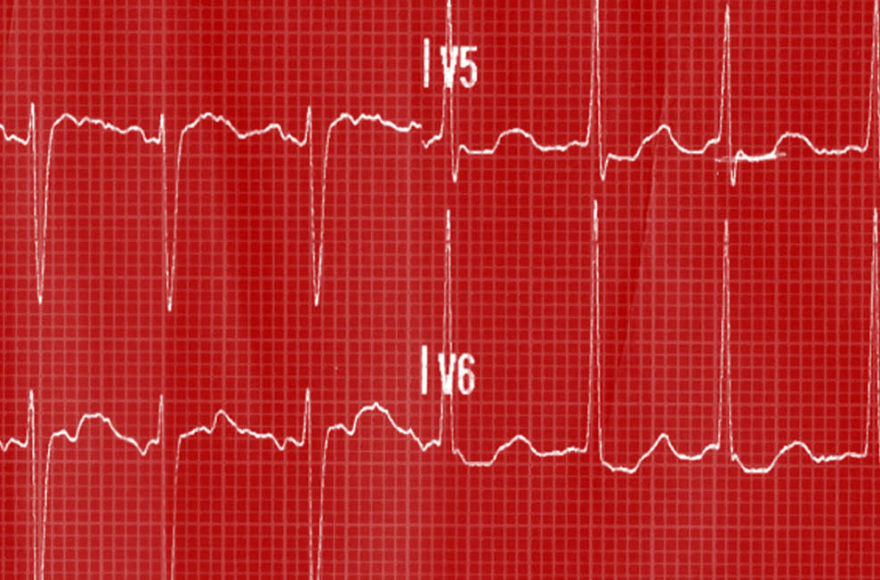
The rhythm strip was printed:

It was regular, not differing R wave heights (as annotated) and no definitive p-waves. They are there but they’re kind of buried within the start of the QRS. So far, so good for an atrial flutter diagnosis.
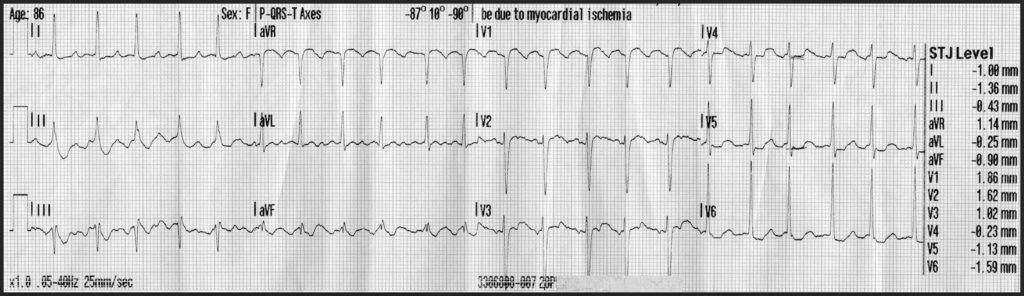
And there we go, a nice flutter pattern, seen best in aVL. Note the depression in V4-V6 which could be rate-related but more suited to the left ventricle enlargement pattern.
Learning Point
This is a nice example how the pre-ECG assessment of the pt can give you a picture of what to expect when the 12-lead prints out.